Cervicogenic headache is one of the most mismanaged conditions in musculoskeletal practice. Patients are cycled through physiotherapy, chiropractic manipulation, and progressive analgesic protocols, all directed at the neck or the head, while the underlying neurological failure remains entirely unaddressed. The cervical spine is the primary structure receiving treatment. The motor neuron supplying the muscles that protect that spine is never tested.
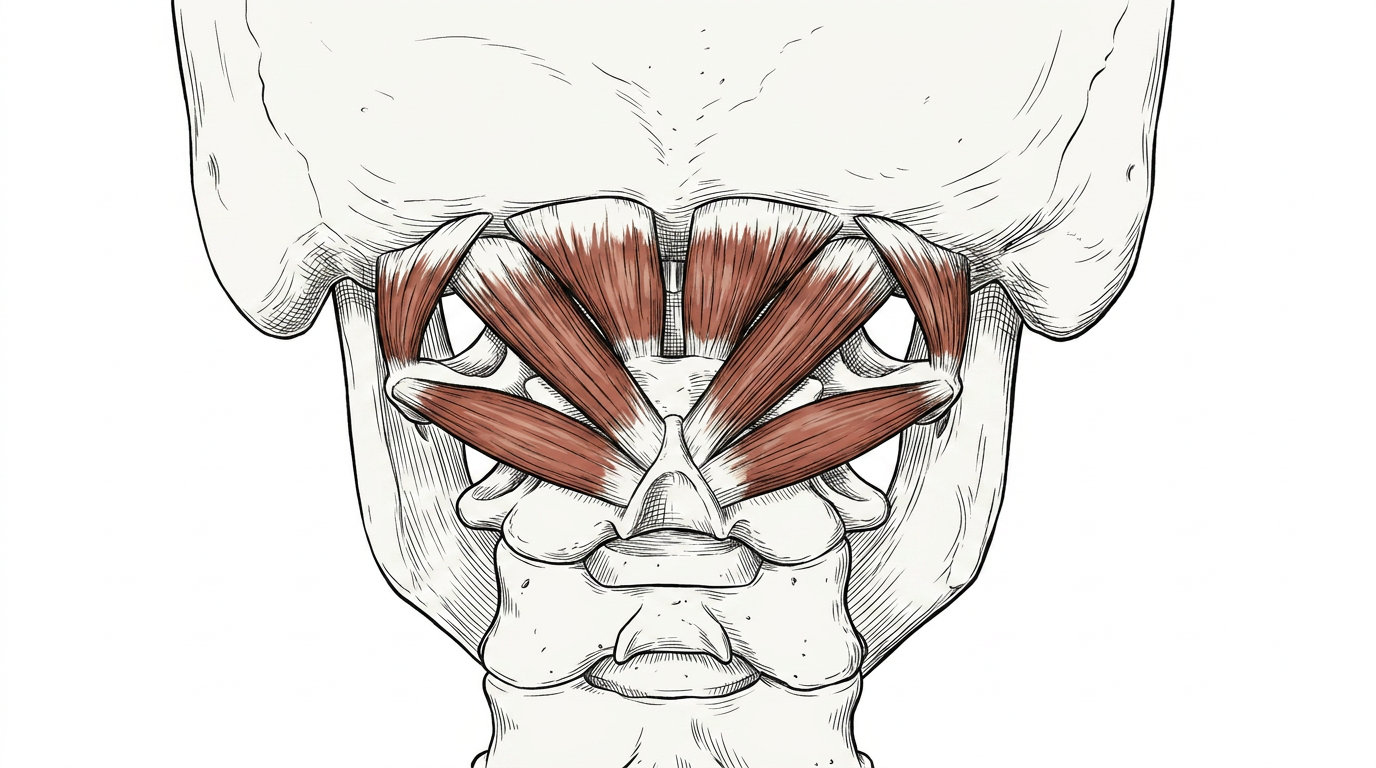
Afferentology asks a prior question: what was the suboccipital musculature doing before the headache appeared? These four small muscles — the rectus capitis posterior major, rectus capitis posterior minor, obliquus capitis superior, and obliquus capitis inferior — are not simply postural muscles. They are the primary afferent transducers of the upper cervical spine, packed with muscle spindles at a density that exceeds almost any other muscle in the body. Their function is precision positioning of the head in three-dimensional space. When they are inhibited, that function disappears — and the consequences propagate both into the joint and into the head.
The Suboccipital Complex: Afferent Density and the Cost of Inhibition
The suboccipital muscles maintain a continuous 50Hz resting tone that provides the cerebellum and brainstem with a constant stream of positional data. This resting tone is not voluntary; it is maintained by the myotatic reflex arc, which responds moment-to-moment to changes in cervical load and position. When an afferent irritant from a remote source — dental occlusion, a cranial suture under stress, or a cervical disc — corrupts this arc, the motor neuron output to the suboccipitals is reduced. The muscles lose their resting tone. The withdrawal reflex pattern that replaces it tends to facilitate the superficial cervical extensors — the semispinalis, splenius capitis, and upper trapezius — which brace the head in compensation, producing the sustained muscular tension that the patient experiences as headache.
What standard assessment misses entirely is the distinction between a muscle that tests weak because it is deconditioned and a muscle that tests weak because its motor neuron supply has been partially withdrawn. Imaging does not show this. Manual muscle testing that is not neurologically precise does not distinguish it. The patient presents with neck stiffness and occipital pain, and the clinician sees a stiff neck and occipital pain — and treats exactly that, while the neurological failure that produced it continues unchallenged.
"The headache is not the problem. It is the readout from a cervical spine that has lost its primary muscular protection. The suboccipitals are offline. Everything else is compensation."
What Is Driving the Inhibition
The afferent inputs that most commonly inhibit the suboccipital musculature include sources the patient would never associate with a headache:
- dental occlusion and bite mechanics: The trigeminal nerve carries sensory input from the teeth and temporomandibular joint directly to the brainstem. An asymmetric bite or a recent dental procedure creates an afferent imbalance that the spinal cord interprets as a threat signal. The withdrawal reflex response inhibits the ipsilateral suboccipitals and facilitates the superficial cervical musculature — producing exactly the clinical picture of cervicogenic headache without a single structural cervical lesion.
- Cranial suture mechanoreceptors: The sutures of the cranium contain mechanoreceptors. Compressive or shear forces on these structures — from a fall, a whiplash event, or even prolonged jaw clenching — generate afferent input that modulates suboccipital tone directly via the suboccipital nerve and the posterior primary rami of C1 and C2.
- Upper cervical disc and facet afferents: The C2-3 facet joint and the C1-2 articulation are richly innervated. Inflammation or mechanical stress at these levels produces afferent input that inhibits the local musculature through segmental withdrawal reflex pathways — a neurological response that precedes and frequently exceeds any structural change visible on imaging.
- Remote scar tissue: Surgical or traumatic scars anywhere in the cervical or cranial region contain mechanoreceptors that, as the scar matures, generate a continuous low-level threat signal. This signal enters the spinal cord and, via propriospinal tracts, modulates motor neuron output to muscles that share the same cord segment — including the suboccipitals.
The Software Test: Precision Muscle Testing
Precision Muscle Testing (PMT) of the suboccipital complex assesses the integrity of the motor neuron supply to these muscles, not simply their contractile force. The practitioner tests the four suboccipitals individually, noting which are inhibited and in what pattern. With the inhibition pattern mapped, a systematic afferent challenge is applied — introducing sensory input from a suspected source and immediately retesting the inhibited muscle. If the muscle restores to full tone with a specific afferent challenge, the source has been identified. This is the Neurological Voltmeter in action: using the motor system as a read-out device for the afferent system.
When the correct source is found and the afferent input is normalised, the suboccipital tone restores immediately. The patient typically experiences an immediate reduction in cervical stiffness and headache intensity. This is not a treatment effect — it is a diagnostic confirmation. The contrast with conventional assessment could not be starker: no imaging modality, no standard orthopaedic test, and no pain scale captures this neurological restoration in real time.
Clinical Takeaways
- The suboccipitals are the primary protectors of the upper cervical spine: Their inhibition creates mechanical vulnerability that leads to joint stress, capsular irritation, and referred pain into the head. The headache is downstream of the neurological failure, not upstream of it.
- The source is rarely at the level of the symptom: Dental and cranial inputs are among the most common afferent drivers of suboccipital inhibition. A patient presenting with cervicogenic headache should be assessed for occlusal asymmetry, recent dental work, and cranial trauma history before the cervical spine is treated as a primary source.
- Imaging does not show neurological inhibition: A normal cervical MRI does not exclude a suboccipital motor neuron problem. A patient with pristine imaging and disabling cervicogenic headache is demonstrating a software failure, not a hardware failure.
- Restoring afferent input restores tone immediately: The correct clinical intervention addresses the afferent source, not the symptom site. When the source is correctly identified via PMT, tone restoration is immediate, objective, and reproducible — distinguishing it from every symptomatic treatment in the conventional toolkit.
Cervicogenic headache is not a neck problem. It is a neurological failure with a precisely identifiable source.
The suboccipital muscles are offline. The joint is unprotected. The headache follows. Finding the afferent source — whether dental, cranial, or discal — and restoring the motor neuron output to these muscles is the only intervention that addresses the condition at its origin. Everything else is pain management.
Learn to enhance your patients' robustness by putting Afferentology into your practice. →
References
- Peck, D., Buxton, D. F., & Nitz, A. (1984). A comparison of muscle spindle concentrations in large and small muscles of the nuchal region of the rat. Journal of Morphology, 180(3), 243-252. (See also: Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of humans. Neurology India, 49(4), 355-359). Adrian, E. D., & Bronk, D. W. (1929). The discharge of impulses in motor nerve fibres: Part II. The frequency of discharge in reflex and voluntary contractions. The Journal of Physiology, 67(2), 119-151.
- Bartsch, T., & Goadsby, P. J. (2003). The trigeminocervical complex and migraine: current concepts and synthesis. Brain, 126(11), 2270-2285.
- Mao, J. J. (2002). Mechanobiology of craniofacial sutures. Journal of Dental Research, 81(12), 810-816.
- Eccles, J. C. (1957). The Physiology of Nerve Cells. Johns Hopkins University Press. (Specifically addressing the central integrative state of the spinal motor neuron).