When a disc herniates, the explanation offered to patients is almost always mechanical. Too much load, a weakened annulus, an unlucky twist. The treatment that follows is equally mechanical: rest, anti-inflammatories, physiotherapy, and if none of that works, surgery to remove the offending tissue. For many patients, the disc heals and the pain remains. For others, the next disc goes six months later.
Afferentology asks a question that precedes all of this: why were the muscles protecting that disc not doing their job? A disc does not herniate in a well-supported spine. It herniates when the reflexes which control muscle tone have been compromised and that compromise has a traceable, identifiable source.
The Deep Stabilisers: Software-Dependent from the Ground Up
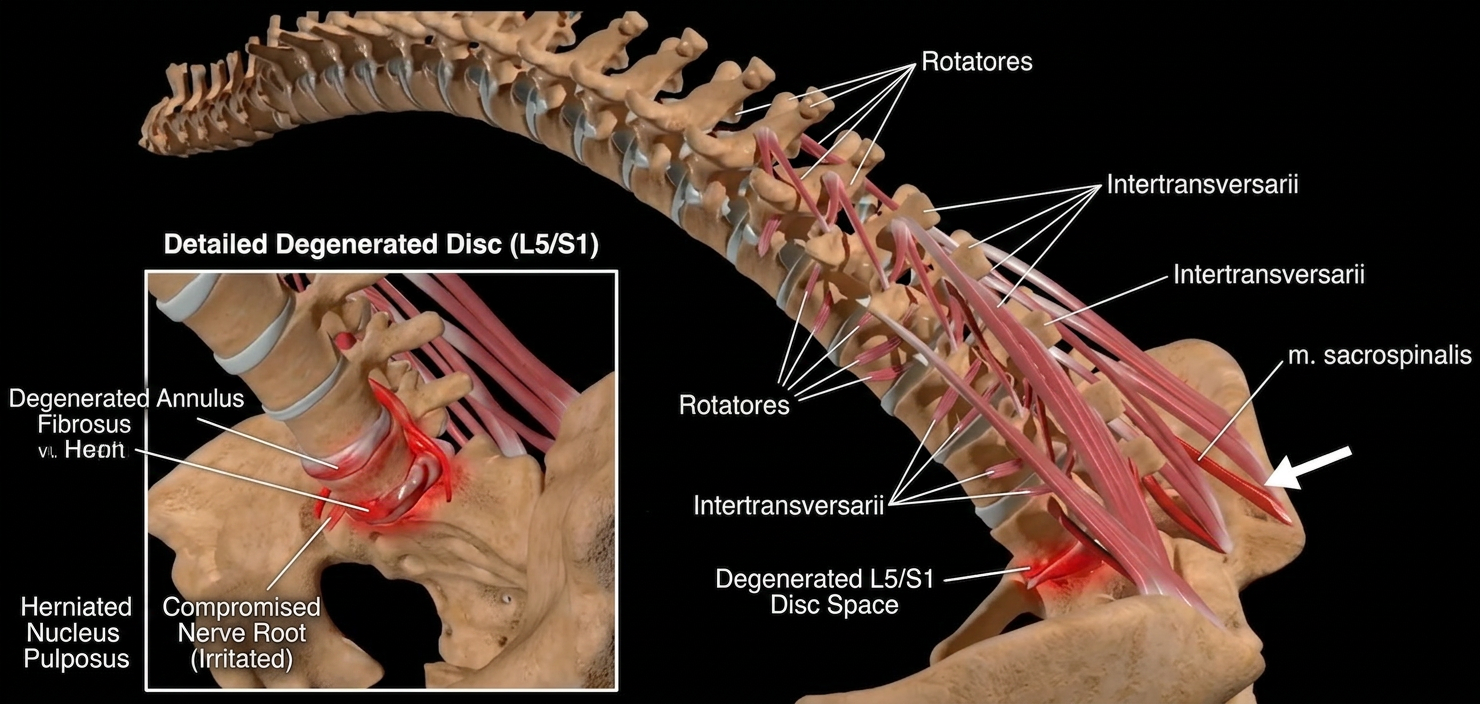
The intervertebral disc is a passive structure. It has no contractile tissue, no motor neurons, no capacity to protect itself. Its protection comes entirely from the deep spinal musculature — multifidus, rotatores, intertransversarii — muscles whose function is governed not by conscious effort but by the 50hz resting tone: the continuous stream of afferent data and efferent control flowing between muscle spindles and the spinal cord motor neurons.
When this signal is clean, the deep stabilisers maintain constant segmental control. Each vertebral level is held precisely in its optimal position under load, and the disc is never asked to absorb forces it was not designed to manage alone. But when the spinal cord detects threat data from an afferent source anywhere in the body it executes a withdrawal reflex resulting in contraction of some muscles and inhibition of others. It reduces the responsiveness of the muscles that are needed for stabilisation and protection of the disc.
"A disc herniation is not the beginning of the problem. It is the mechanical damage at the end of a neurological process that began with a bad input. The disc failed because the protective reflexes that should have been protecting it had already been compromised."
What Triggers the Reflex Before the Disc Goes
The afferent irritants most commonly driving deep lumbar stabiliser inhibition are not dramatic. They are quiet, persistent signals the nervous system has learned to accommodate during normal function but over time, leads to degenerative change and may fail suddenly under excessive or unexpected loading. Common sources include:
- Scars: Skin receptors are very sensitive. They can feel one hair move and can activate muscles appropriately - to rub an injury, scratch an itch or swat a mosquito. Surgical or non-surgical scars can create ongoing mechanoreceptor activation that the spinal cord interprets as an irritation. The response may be inhibition of the muscular stabilisers at the relevant spinal levels.
- Anterior abdominal and pelvic scars: C-section and appendectomy scars trigger a withdrawal reflex that inhibits the lumbar extensors and multifidus on the ipsilateral side — a neurological bracing of the anterior wall that leaves the posterior unprotected.
- dental afferent irritants: Root-filled teeth, poorly fitted crowns, and amalgam restorations may produce abnormal afferent signals that propagate into the motor cortex, selectively reducing tone in the deep paraspinal muscles across multiple lumbar levels.
- Disc annulus proprioceptors: Once a disc is injured, the mechanoreceptors within the annulus fibrosus can refer pain to surrounding areas. This is why discogenic pain is so resistant to conservative care that does not address afferent input and muscular control.
The Software Test: Resilience Muscle Testing
Standard imaging shows the herniation. It does not show why the multifidus at that level had insufficient tone to prevent it. Precision Muscle Testing approaches this gap by using the muscle as a Neurological Voltmeter, a real-time readout of the spinal cord's current output at that segment.
The practitioner tests the tone of the deep stabilisers, then systematically challenges candidate afferent sources: pressing on a scar, making dental contact, removing a piece of jewellery. When the previously inhibited muscle restores full tone in response to a specific input, the source of the withdrawal reflex has been identified. The treatment is not the muscle test, it is the removal or neutralisation of the irritant. The muscle tone returns because the software bug has been remedied, not because the hardware has been repaired. However, clinical improvement is often noted even if the disc has not had time to repair, because the disc has returned to a state of stability and control. Pain is reduced and if repair is possible, it is now able to proceed.
Clinical Takeaways
- Disc herniations are a neurological event before they are a structural one. The muscle inhibition that leaves the disc unprotected precedes the injury and must be addressed to prevent recurrence.
- Imaging the disc without auditing the afferent system is incomplete diagnosis. The herniation is visible; the cause is not, unless you know how to look for it.
- Post-injury annular proprioceptors perpetuate the reflex. Injured discs become their own afferent irritants, maintaining the withdrawal reflex that caused the injury. This cycle must be broken neurologically, not mechanically.
- Recurrent disc injury follows unresolved secondary muscle inhibition. Patients who re-herniate at the same or adjacent levels have not had their aberrant afferent source identified. The disc is not the weak link — the control system is.
The Disc Didn't Fail. The System Did.
Treat the disc and you manage the consequence. Find the withdrawal reflex and you address the cause. Every patient with a disc herniation deserves a neurological audit before any structural intervention — not because it replaces imaging or surgery when genuinely needed, but because without it, the next disc is already at risk.
Learn how to accurately diagnose disc lesions and the other common causes of low back pain. →