We have been taught to look at osteoarthritis as a simple "wear-and-tear" problem—a mechanical countdown where joint cartilage inevitably grinds away under the weight of time and gravity. But groundbreaking biomechanical research reveals a deeper, more empowering truth: your cartilage isn't failing from a lack of structural durability, but because its primary muscular shield has been neurologically throttled.
The Herzog Experiments: Proving the Muscular Cause of Joint Decay
For decades, orthopaedic medicine assumed that muscle weakness was merely a downstream side effect of arthritis—that a painful, inflamed joint naturally caused a patient to stop using their limbs, leading to muscle atrophy. However, a series of elegant, milestone experiments conducted by Dr. Walter Herzog and his team at the University of Calgary completely flipped this cause-and-effect model on its head.
Instead of surgically damaging joints to observe how they degenerated, Herzog’s researchers used periodic injections of botulinum toxin type A to selectively paralyse and weaken the quadriceps muscles in rabbits. The joints themselves were left entirely untouched. Within just four weeks of inducing a 60% to 80% drop in muscular force generation, the researchers observed a catastrophic onset of osteoarthritic changes. The femoral condyles and tibial plateaus displayed widespread cartilage thinning, cellular cloning, and surface fibrillation.
The implications of this animal model cannot be overstated: the structural cartilage matrix failed not from systemic disease or old age, but because the active muscular motor supply was turned down. The joint was left completely exposed to unmitigated, unpredictable micro-translations during movement. In short, the muscular weakness was the upstream cause; the structural decay was the downstream consequence.
The 50hz Baseline and the True Protection of the Knee
In a healthy musculoskeletal framework, every muscle operates with an automated, involuntary 50Hz resting tone. This continuous electrical background hum acts as a stabilizer, adjusting tension moment-by-moment via the myotatic reflex arc to keep joints centered and safe. When an afferent sensory insult—whether an old scar, a surgical injury, or a structural irritant—floods the spinal cord with data, the central nervous system responds with an involuntary withdrawal reflex. It dials down the motor neuron output below that healthy 50Hz threshold, inhibiting the prime movers.
The Hardware vs. Software Distinction: Standard medical treatments view the narrowing of a knee joint as a "hardware" issue, focusing entirely on the worn cartilage or bone spurs. Afferentology recognizes that the joint space narrowing is actually the result of a "software" glitch. The quadriceps act as the primary kinetic shock absorbers for the lower limb, neutralizing up to 70% of the impact forces generated when your foot hits the ground. When software inhibition takes those muscles offline, the unbuffered mechanical stress is transferred straight into the articular cartilage.
Large-scale human clinical trials, such as the Multicenter Osteoarthritis Study (MOST), have validated Herzog's findings in human populations. Researchers tracking thousands of adults discovered that baseline quadriceps weakness accurately predicted the future development of knee joint space narrowing and chronic pain years before radiological changes ever appeared on an X-ray. The joint cartilage doesn't simply wear out; it is actively crushed because its defensive software shield has been deactivated.
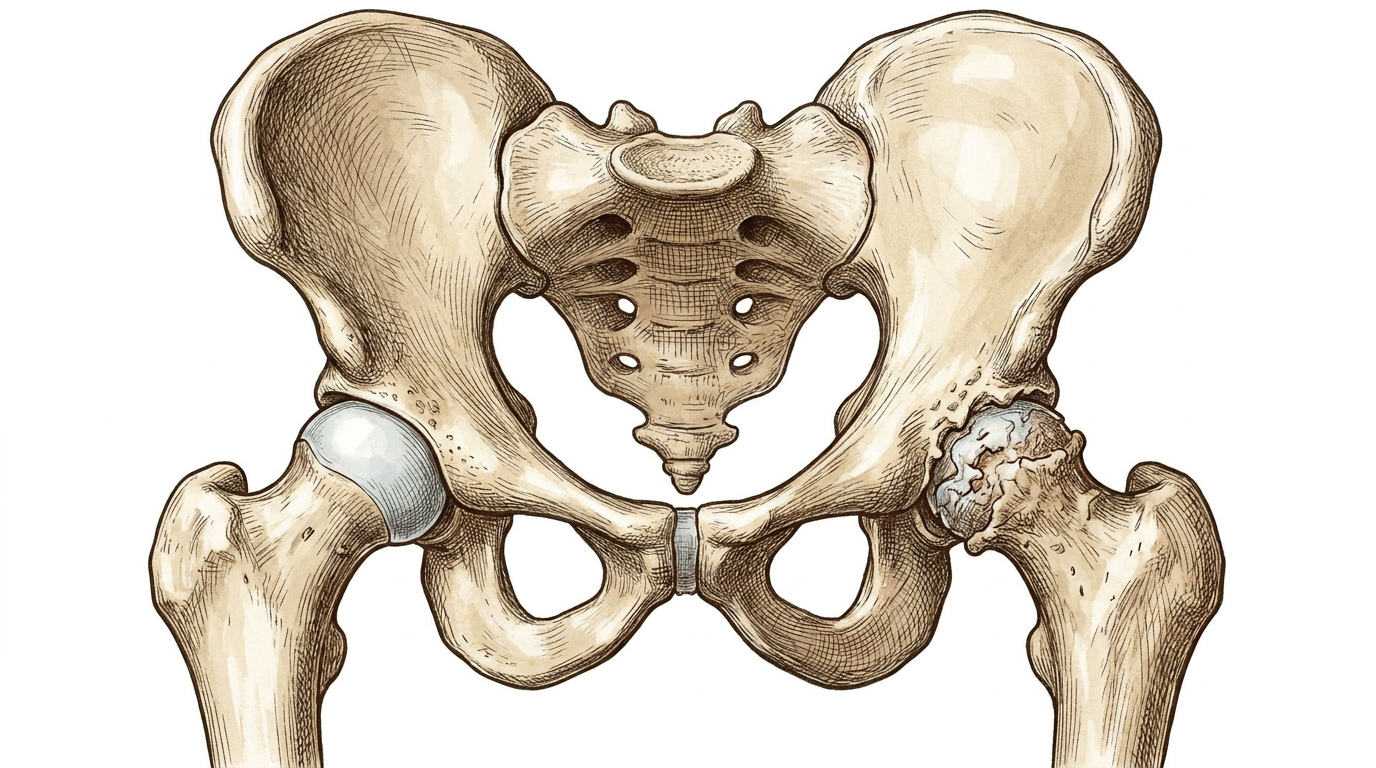
Gluteus Maximus Inhibition and the Destruction of the Hip
This exact same neurological breakdown governs the degradation of the hip joint. While conventional orthopedics treats hip osteoarthritis with localized injections or joint replacements, a deeper look at the surrounding musculature reveals a predictable pattern of motor neuron withdrawal. The gluteus maximus is the primary mechanical governor of the hip, responsible for driving extension and keeping the femoral head safely centered within the acetabulum during locomotion.
When an afferent irritant triggers a withdrawal reflex that inhibits the gluteus maximus, the muscle loses its capability to manage unpredictable external forces. Without the robust control of the glutes, the femoral head begins to migrate anteriorly and superiorly during every single step. This subtle, repetitive structural shift creates localized high-pressure zones, overloading the delicate anterior labrum and wearing away the protective cartilage matrix. By the time a patient is diagnosed with hip arthritis on a pelvic film, they have typically endured a decade of hidden muscular inhibition that standard orthopedic assessments never evaluated.
The Nail in the Foot Analogy: Trying to treat hip or knee arthritis by focusing solely on strengthening the quadriceps or glutes through repetitive exercise is like trying to run with a nail in your foot. The brain's survival programming will always choose protection over power; it will actively inhibit those muscles to protect the body from what it perceives as an ongoing threat. No amount of rehabilitation can override this hardwired protective withdrawal reflex until the underlying sensory short-circuit is found and removed.
Clinical Takeaways for Restoring Structural Longevity
- Muscle weakness is a primary driver, not a symptom: Neurological inhibition of the quadriceps and gluteal muscles frequently precedes the structural degradation of the knee and hip joints by years or decades.
- Exercise cannot override an active withdrawal reflex: Forcing a patient to perform heavy resistance rehabilitation into an actively inhibited muscle will only cause further compensation, joint strain, and accelerated wear.
- X-rays and MRIs show the aftermath, not the cause: Diagnostic imaging is an exceptional tool for inspecting hardware damage, but it is completely blind to the 50Hz software baseline failure that permitted the damage to happen.
- True joint protection requires sensory clearing: By utilizing Precision Muscle Testing to identify and clear hidden sensory irritants, you instantly restore the baseline motor neuron supply, re-establishing the joint's natural shield against unpredictable force.
Joint degeneration is not an inevitability of aging. It is the predictable outcome of an unprotected structural framework.
When the software fails, the hardware breaks down. By shifting your perspective from chasing arthritic wear-and-tear to identifying and facilitating inhibited muscles, you stop managing symptomatic noise and begin restoring true, long-term functional robustness.
References
- Herzog, W., Longino, D., & Clark, A. (2003). The role of muscles in joint adaptation and degeneration. Langenbecks Archives of Surgery, 388(5), 305-315.
- Rehan Youssef, A., Longino, D., Seerattan, R., Leonard, T., & Herzog, W. (2009). Muscle weakness causes joint degeneration in rabbits. Osteoarthritis and Cartilage, 17(9), 1228-1235.
- Longino, D., Frank, C., & Herzog, W. (2005). Acute botulinum toxin-induced muscle weakness in the anterior cruciate ligament-deficient rabbit. Journal of Orthopaedic Research, 23(6), 1404-1410.
- Segal, N. A., Torner, J. C., Felson, D., Niu, J., Sharma, L., Lewis, C. E., & Nevitt, M. (2009). Effect of thigh strength on incident radiographic and symptomatic knee osteoarthritis in a longitudinal cohort. Arthritis & Rheumatism, 61(9), 1210-1217.
- Slemenda, C., Heilman, D. K., Brandt, K. D., Katz, B. P., Mazzuca, S. A., Braunstein, E. M., & Byrd, D. (1998). Reduced quadriceps strength relative to body weight: a risk factor for knee osteoarthritis in women? Arthritis & Rheumatism, 41(11), 1951-1959.
- Loureiro, A., Mills, P. M., & Barrett, R. S. (2013). Muscle weakness in hip osteoarthritis: a systematic review. Arthritis Care & Research, 65(3), 340-352.
- Grimaldi, A., Richardson, C., Durbridge, G., Donnelly, W., Darnell, R., & Hides, J. (2009). The association between degenerative hip joint pathology and size of the gluteus maximus and tensor fascia lata muscles. Manual Therapy, 14(6), 611-617.