We usually think about muscle tone in terms of movement. Strong muscles protect joints. Weak muscles allow injury. The rehabilitation model is built on this premise: identify the weak muscle, load it progressively, restore its strength. This is not wrong. But it is profoundly incomplete. The animal neurophysiology of the last four decades reveals something that structural medicine has not yet integrated: muscle tone is not just the mechanical guardian of the skeleton. It is the primary afferent signal that governs the sympathetic drive to the body''s organs and glands. Switch the muscles off for any reason and you do not just destabilise joints. You disrupt adrenal function, kidney regulation, blood pressure control, hormonal output, and the basic metabolic machinery that keeps a person energised and functional.
This is not theory. It is experimental data from peer-reviewed neurophysiology. The clinical implications are vast and almost entirely unexplored in mainstream practice.
What Two Key Studies Established
Two papers, published in 1989 and 1991, changed what we should understand about the relationship between muscle and organ function, although medicine has been slow to apply the finding.
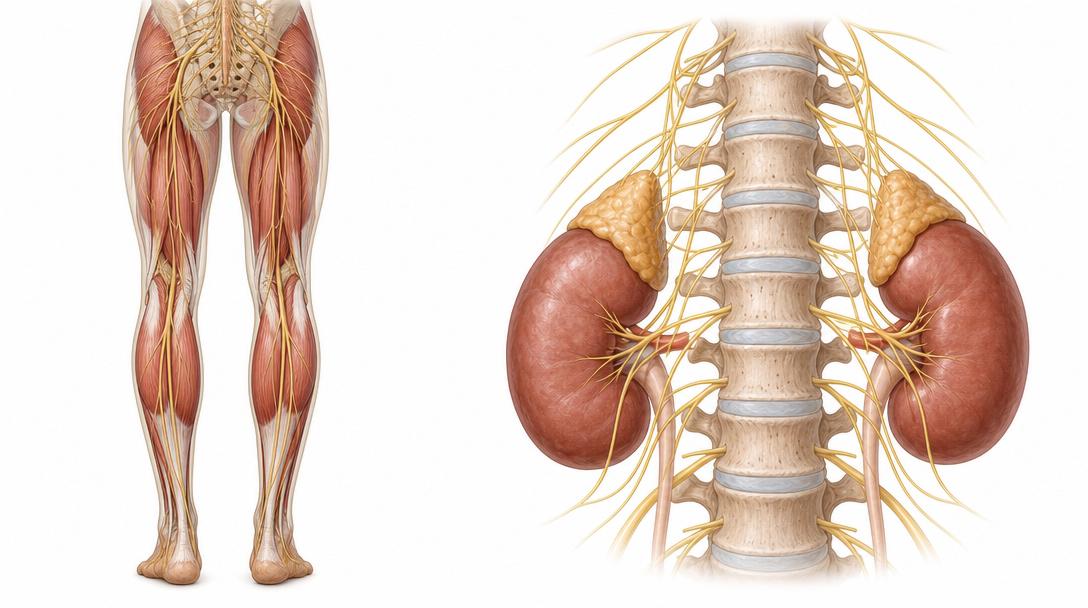
Victor and colleagues demonstrated in anesthetised cats that static contraction of the calf muscle tripled renal sympathetic nerve activity within three seconds of onset. The response was abolished when the L6 and S2 dorsal nerve roots were severed. These are the nerves carrying messages from the muscles to the spinal cord from the contracting muscles. The conclusion was direct: mechanoreceptors with group III afferents (muscle spindles) reflexly drive sympathetic outflow to the kidney. The kidney's nervous system input comes from the muscles.
Two years later, the same research group refined the technique and inserted microelectrodes into the sympathetic nerve supply of the adrenal glands in rats. The result was equally unambiguous: static muscle contraction reflexly increases sympathetic nerve activity to the adrenal gland. The pathway is the same. Muscle spindle afferents into the spinal cord, sympathetic outflow to the adrenal medulla. The adrenal gland produces more adrenaline because the muscles told it to.
"Muscle tone is not just the scaffolding that holds the skeleton together. It is the driver of afferent signals that tell the adrenal glands to drive you, tells the kidneys to regulate your blood pressure, and provides the continuous neurological instruction that keeps your metabolic machinery running. Inhibit the muscles and you inhibit the organs."
The Dental Crown That Changed Everything
Consider a patient who sees a dentist for a crown. The procedure is routine. But the crown introduces a slight occlusal interference, a new contact point that the trigeminal nerve registers as an anomaly. The nervous system, interpreting this as an afferent threat, initiates a withdrawal reflex. Cortical drive to specific muscle groups is reduced. The leg muscles, particularly on the ipsilateral side lose tone. Their spindle output drops.
Within days, the patient notices they are tired. Their blood pressure, checked at a follow-up, has crept up. They lack their usual energy and drive. Every investigation comes back within normal limits. The adrenal gland looks fine on paper. The kidneys appear healthy. What no investigation is showing is that the sympathetic nerve signal to both of these organs, the signal that comes entirely from muscle spindle afferents, has been diminished by a dental afferent input that switched the muscles partially off.
This is not a hypothetical. It is the direct application of the neurophysiology. The mechanism is established. The clinical presentation follows from it precisely.
The Organs and Glands That Depend on This Signal
The adrenal gland and the kidney are the two organs most clearly demonstrated in the literature to receive sympathetic drive via the muscle spindle reflex. But they are unlikely to be the only ones. The sympathetic nervous system governs a broad range of organ functions through spinal pathways that are subject to the same afferent modulation. The implications extend to:
- Adrenal function and energy regulation: Adrenaline and noradrenaline release is driven by adrenal sympathetic nerve activity. Inhibited muscle tone suppresses this drive. The result is persistent fatigue, blunted stress response, poor motivation, and reduced capacity for sustained effort, presenting identically to "adrenal fatigue" but originating in the afferent input system, not the gland.
- Kidney function and blood pressure: Renal sympathetic nerve activity governs fluid handling, renin release, and vascular resistance. Suppressed spindle input disrupts this regulation. Blood pressure rises not because the kidney is diseased but because its neurological instruction has been degraded.
- Hormonal cascades: The sympathoadrenal axis sits at the head of a hormonal cascade. When adrenal output is suppressed by reduced spindle afferent drive, the downstream effects include disrupted cortisol rhythms, impaired thyroid axis modulation, and altered sex hormone balance — all of which can present as metabolic dysfunction without any primary glandular pathology.
- Immune regulation: Sympathetic innervation of lymphoid tissue and immune organs is well established. The same spindle-driven sympathetic pathways that govern adrenal and renal function are likely to influence immune tone, potentially explaining the immune dysregulation seen in patients with chronic withdrawal patterns.
Why Exercise Works — and Why It Is Not Enough
The research on exercise and both blood pressure and fatigue is consistent: physical activity improves both. The mechanism, viewed through this lens, is straightforward. Exercise activates muscle spindles. Spindle afferents drive sympathetic outflow to the adrenal glands and kidneys. Organ function improves. The patient feels better and their blood pressure comes down.
But exercise is a temporary restoration of a signal, not a correction of the source of its suppression. The patient who exercises regularly but still carries an active withdrawal reflex from a scar, a dental focus or a foreign body is compensating for an afferent problem rather than resolving it. They feel well when they exercise and less well when they stop. The underlying withdrawal remains. The organs are still waiting for a signal that is only being provided intermittently.
Clinical Takeaways
- Muscle tone is an organ regulation signal, not just a structural variable. Every clinical assessment should evaluate muscle tone as a proxy for the quality of sympathetic drive to the adrenal glands, kidneys, and other organ systems, not just as a measure of joint stability.
- Unexplained fatigue, blood pressure changes, and hormonal dysregulation are afferent questions. Before investigating the organ, investigate the input the organ depends on. If muscle tone is inhibited, the organs cannot receive appropriate sympathetic drive regardless of how well they function structurally.
- The history reveals the source. When did the fatigue begin? When did the blood pressure start rising? What happened in the weeks prior? Dental work, surgery, an injury, a new piercing? The onset is a clinical pointer to the afferent event that initiated the withdrawal reflex.
- Restoring muscle tone is organ medicine. When the withdrawal reflex is identified and its source removed, muscle tone returns immediately. The spindle afferent signal is restored. Adrenal and renal sympathetic drive resumes. This is not an indirect effect. It is the direct restoration of the neurological pathway the organs depend on.
Muscle Tone Is the Beginning and the End of the Nervous System.
The skeleton holds the body upright. The muscles make it move. But they also tell the adrenal glands to drive you, tell the kidneys to regulate your pressure, and provide the afferent instruction that keeps the body's metabolic machinery running, continuously, reflexly, without conscious direction. This is not supplementary to their musculoskeletal role. It is inseparable from it. A body with inhibited muscle tone is not just at risk of injury. It is an organism whose organs are receiving a degraded instruction signal and trying to compensate for it in every way available. Find the inhibition. Restore the tone. Everything else follows.
Learn to apply Resilience Muscle Testing in your practice. Explore the Afferentology courses. →
References
- Vissing, J., Wilson, L. B., Mitchell, J. H., & Victor, R. G. (1991). Static muscle contraction reflexly increases adrenal sympathetic nerve activity in rats. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology, 261(5), R1307-R1312. https://doi.org/10.1152/ajpregu.1991.261.5.R1307
- Victor RG, Rotto DM, Pryor SL, Kaufman MP. (1991). Stimulation of renal sympathetic activity by static contraction: evidence for mechanoreceptor-induced reflexes from skeletal muscle. Neuroscience, 12(1), 289-299. Circ Res. 1989;64(3):592-599.