In July 2008, a landmark study published in the British Medical Journal (BMJ) sent shockwaves through the health community. Researchers established a direct association between muscle strength and mortality—unrelated to fitness or exercise levels. The data was clear: men in the weakest third were 33% more likely to die from all causes. For men over 60, the strongest third enjoyed half the mortality rate of the weakest.
This study suggests that strength isn't just about the "hardware" of muscles; it is a clinical marker of systemic integrity. A year later, I decided to put the Afferentology model to the test. If chronic weakness is a "software" glitch caused by inhibited neurological signals, could a clinical intervention alter these life-determining ratios?
The Protocol: Measuring the Strength-to-Mass Ratio
To replicate the BMJ study, I had to account for the fact that a 120 kg man is naturally stronger than a 70 kg man. The key is the ratio of strength per kg of muscle mass.
Using a Bioscan 916 (Maltron) for bioelectrical impedance, I accurately measured muscle mass. To measure output, I utilized a one-rep maximum (1RM) on the bench press and a deadlift (replacing the standard leg press to ensure height and knee angles didn't skew the results). By combining these lifts and dividing by muscle mass, I established a baseline of "Neurological Efficiency."
Watch the Experiment in Action:
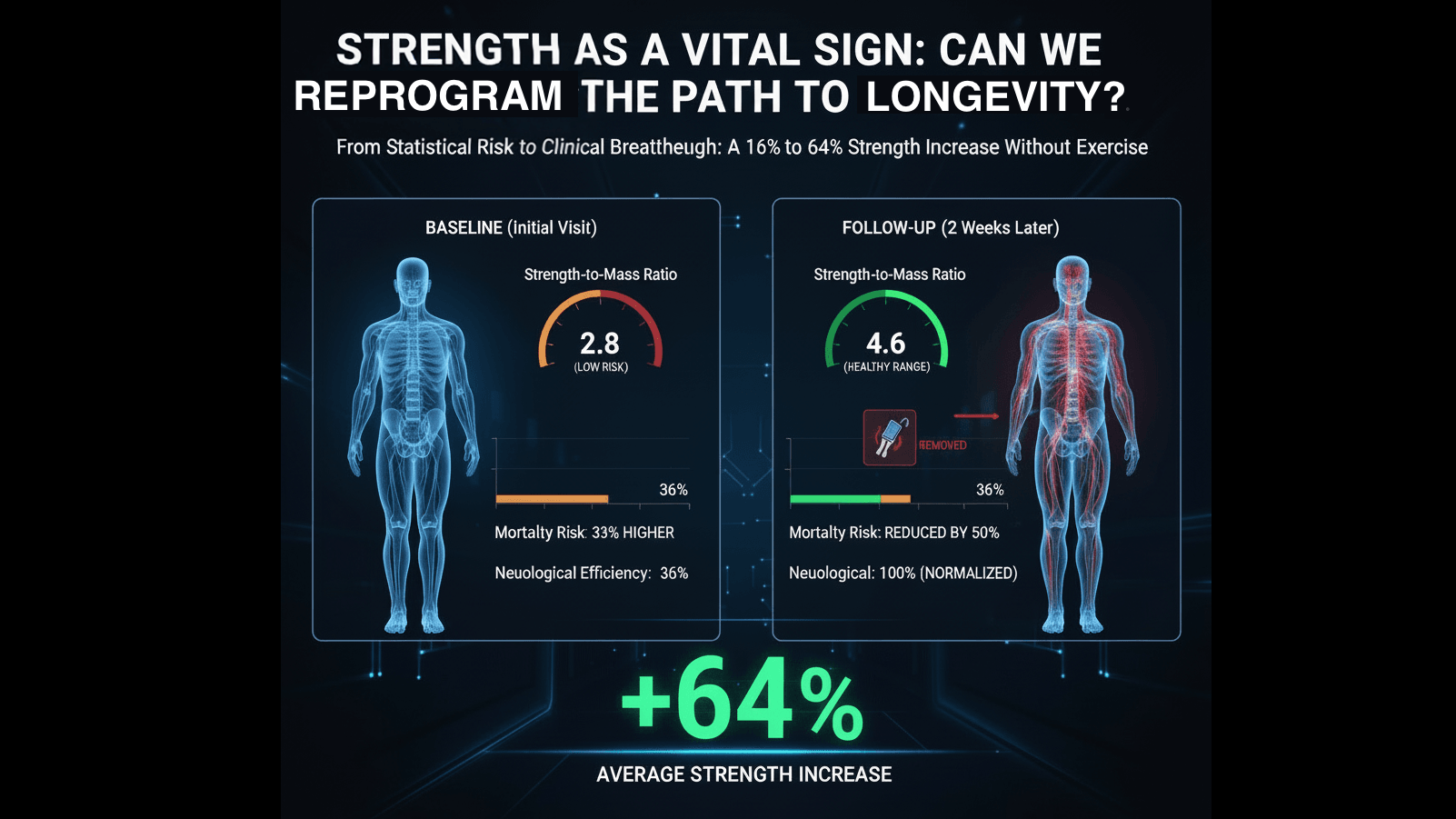
The Results: Beyond the "Danger Zone"
I tracked 100 consecutive patients, re-measuring their ratios within two weeks of their initial treatment. The goal was to see if correcting afferent irritants—those neurological "nails in the foot"—would immediately unlock suppressed strength.
The findings were extraordinary:
| Patient Group | Baseline Strength Ratio | Average Strength Increase |
|---|---|---|
| Lowest Third (High Risk) | Below 3.3 (Men) / 2.0 (Women) | 64% |
| Middle Third | Average Range | 17% |
| Top Third (Athletes) | Above 5.0 (Competitive) | 10% |
Critically, every patient in the "lowest third"—those statistically most at risk for early mortality—was lifted out of the danger zone within just two visits. This wasn't the result of hypertrophy or weightlifting; it was the result of removing neurological inhibition.
Conclusion: Restoring the 50Hz Resting Tone
When a patient increases their strength by 64% in two weeks without picking up a dumbbell, we aren't seeing new muscle growth; we are seeing the restoration of normal efferent output. By identifying the faulty inputs causing muscle inhibition, we can fundamentally alter a patient's health trajectory.
While this pilot study deserves a formal control group, the implications are profound: we can measure, and more importantly, fix the weakness that standard medicine simply manages with statistics.